
NO TOPOGRAPHER? NO PROBLEM!
In a perfect world, every eyecare practitioner would have the latest-and-greatest state-of-the-art equipment to help diagnose and manage patients. Of course, this is not realistic, especially if it is not financially appropriate or if you practice in a setting that requires a multitude of paperwork and decision-making from company officials (which could take years). When fitting specialty contact lenses, many practitioners will ask me if they need a topographer to properly fit these lenses. In my opinion, if you are fitting patients with orthokeratology or corneal reshaping lenses, a topographer is definitely necessary to monitor the progress in these patients. But for corneal GP lenses and scleral lenses, there are a variety of opinions out there.
Topographer Alternatives
When I first joined my practice, I wanted to get a topographer right away so I could start seeing specialty contact lens patients. With three locations, it was not financially possible to purchase an expensive piece of equipment like this for all three, so we purchased one only for the main location.
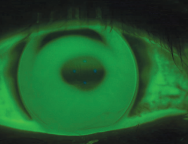
Figure 1. A 6.25mm base curve lens showing heavy apical bearing in a keratoconus patient.
The other two locations did not have a topographer, but I wasn’t going to let this stop me from fitting specialty lenses. My good friend, Dr. Christine Sindt, once told me that the best topographer was a corneal GP lens. She was right.

Figure 2. Global pachymetry showing severe thinning in a post-LASIK patient
I had a 22-year-old male who presented for a comprehensive eye exam, and he complained that his vision OD was blurry and was gradually worsening over time. His refraction showed a large amount of cylinder (with which he stated that the letters still looked doubled), and he had a scissoring reflex with retinoscopy. The cornea did not appear thin on slit lamp exam, and there was no striae.
At that moment, I wished that I had a topographer because I could not verify the corneal shape with the naked eye. However, I took Dr. Sindt’s advice and applied the steepest lens that I had in my spherical GP kit from optometry school (6.25mm base curve). Sure enough, the fluorescein pattern showed heavy apical bearing to confirm the diagnosis of keratoconus (Figure 1). He was later fit with a scleral lens, and he can now see 20/25 without diplopia.
Another tool that I have found useful is my optical coherence tomographer (OCT). The pachymetry feature is very helpful for patients who have suspicious corneas. Once again, without a topographer, this can help determine how thick or thin a patient’s cornea is, which can help lead to a diagnosis. If patients have central thinning, it is possible that they may have an ectatic cornea (Figure 2).
Don’t Be Deterred
If you currently practice in an office without a topographer, you can still fit specialty contact lenses. Use simple spherical GP lenses and assess the pattern to aid in your diagnosis. Your lab of choice can easily and inexpensively manufacture something like this for you without the huge expense of a topographer.
Ideally, we would all love to have topographers to assist in diagnosing and treating patients, but if you are in a setting that does not have the luxury of these machines, don’t let that stop you. Get creative, and you’ll be surprised at how many irregular corneas are out there.